When you ask five companies how much they would charge to build a telemedicine MVP, you receive five different prices, ranging from $15,000 to $400,000. One quote seems very good, while another is five times higher than the lowest one, and there is no explanation for this.



The budget allocated to an MVP depends on two factors. First, the decisions made regarding whether to build the MVP in a compliant manner and/or integrate existing systems into your MVP. Second, the level of support your first 100 patients will require. Our guide details what is bought at each budget level, where cheap quotes mask the true cost, and how to scope an MVP effectively. The feature details provided in this guide are based on actual healthcare projects we have completed.
{{banner-4}}
Why telemedicine startups fail by overbuilding
We see the same pattern on nearly every scoping call. A founder opens a document — often a feature list assembled from competitor products and investor expectations — and much of it is already closer to a second release than an initial one. Things like multi-party video, AI-based diagnostics, or full Epic integration get added early. Even though they all feel essential, together they quietly stretch timelines by months and inflate costs. What’s more, none of them proves that a real clinician will use the product.
Over-scoping the MVP is the single most common reason healthcare products miss their launch window. The teams that win treat the first release as a question: Will a real clinical user adopt this? After answering it, they cut everything that doesn’t help answer it. An effective telehealth MVP is narrow, compliant, and boring in all the right places. Simply put, save the innovation for version two.
On the other hand, there is the cost of rebuilding features if you miss them at the scoping stage and your architecture is set in stone by month 4.
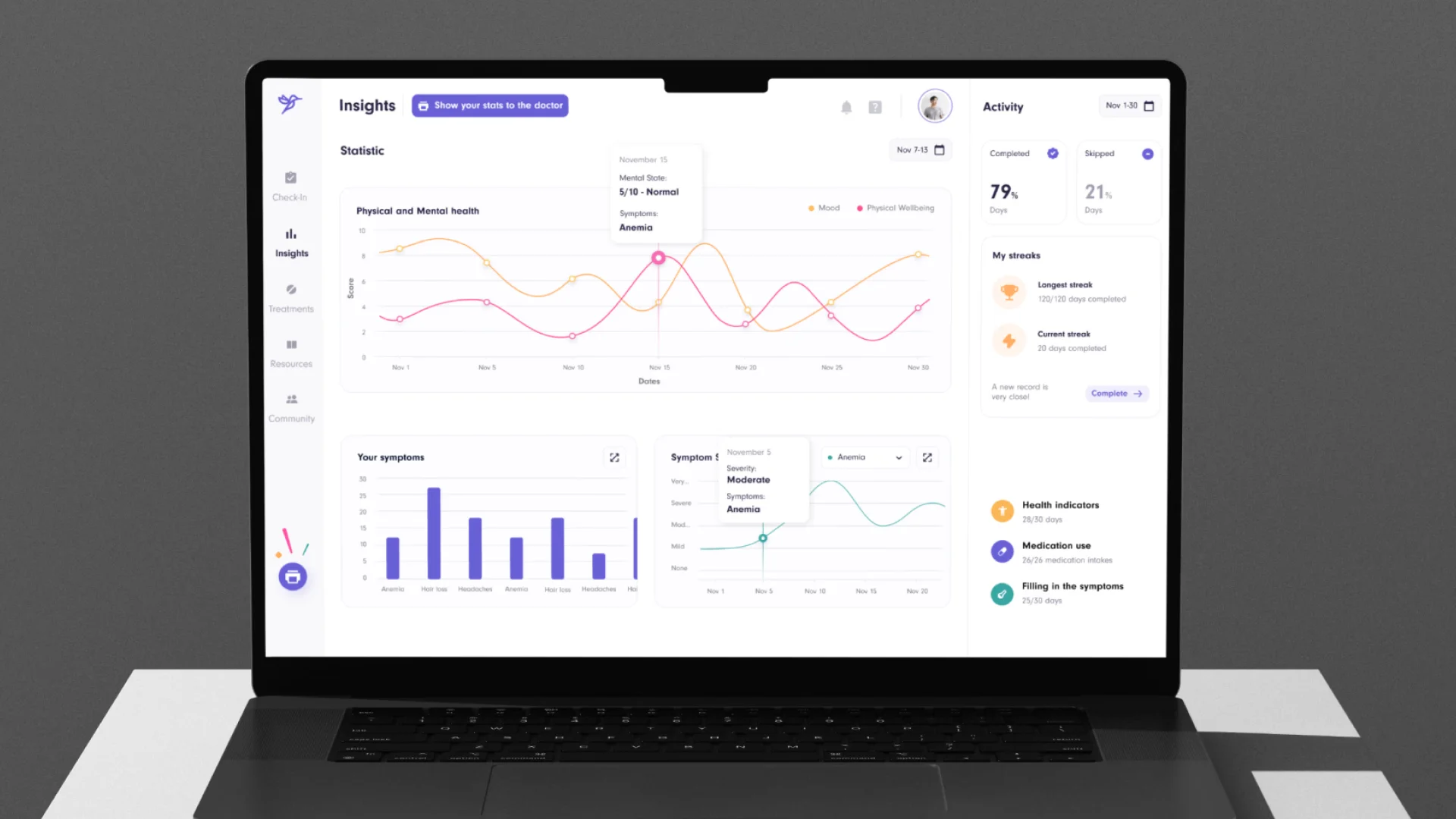
When Halo Lab redesigned MyReha, a neuro-rehabilitation platform for clinicians and family members, for nyra health, we found that the product experience was not keeping up with technological evolution. The reason was that the product moved from tablets to smartphones and from hospital-based care to home care. Their 17-month project involved rebuilding the therapist dashboard around one primary principle: enabling clinicians to determine a patient’s status in seconds, rather than the number of clicks required before the redesign. It is much cheaper to factor in the cost of rework at the outset than to retrofit it later.

A telemedicine MVP: what it is and what it is not
A telemedicine MVP is the smallest version of your platform that can deliver a care journey safely, legally, and well enough that a clinician and a patient will come back to it.
This definition restricts things to those that:
- are considered within the definition (e.g., secure video, encrypted messaging, scheduling, identity and access control, and the compliance structures that will allow you to handle protected health information);
- may not be considered good enough products to be included in the definition (e.g., new specialties, advanced automated capabilities, integrated support for a clinical partner that is not currently requested or expected).
This definition also clarifies what doesn’t qualify. For instance, a telehealth product might just be a scaled-down version of a broader enterprise platform, or simply a proof-of-concept built to demonstrate an idea.
If a telehealth system doesn’t provide a clear way to connect a patient to a real human when something goes wrong, it shouldn’t be called an MVP. In that case, it’s closer to a branded prototype than a usable product. In short, unless patients are actually receiving real care through the system, it doesn’t meet the standard of a telehealth MVP.
The MVP feature scope: patient vs. provider vs. admin
A telemedicine platform is three products wearing one logo. Patients, providers, and administrators each touch a different surface, and each surface has a non-negotiable core. When scoping the MVP, you should decide what the minimum is for all three — then stop.
Essential patient portal features
Traditional patient portals lose a large share of users at the app download stage, so every feature here has to reduce friction, not add it. Here are some things you’ll need to check:
- Secure login and identity. Have unique credentials and access to only your records based on your role when logging into your account. This includes having a straightforward onboarding process.
- Physician directory with filters. It allows the patient to find physicians based on specialty, language spoken, and region. Patients will see a physician’s credentials (licensure, etc.) when they tap that physician’s name, which will help them decide to work with them or not.
- Real-time booking with reminders. Live provider availability, self-booking, automated SMS and email reminders, and clean cancel/reschedule flows. This is one of the fastest operational wins you can ship, as it reliably reduces no-show rates across healthcare contexts.
- HD video consultation, plus the lobby around it. WebRTC with adaptive bitrate, auto-reconnect, and encryption matters, but many overlook the virtual waiting room. This is a pre-call lobby where patients test the camera and mic and watch a countdown instead of staring at silence.
Note: That last point is where founder instinct and patient reality diverge. In nine telehealth builds out of ten, the first feature founders request is multi-party video, and in nine out of ten, the first feature patients actually need is a working pre-call mic check.

Critical doctor dashboard functionalities
If the dashboard adds clicks to providers’ days, they route around it. The clinician core includes:
- Profile and license management. Specialty, license, region, languages, availability, and a credentialing card patients can open mid-call to confirm they’re speaking to a real, licensed clinician.
- Calendar and availability manager. Real-time control over slots, synced to the patient-facing booking system, so double-bookings can’t happen.
- Structured clinical notes. Light note templates from day one. Free-text-only notes become a dead end fast; a little structure now keeps the data usable when you eventually integrate an EHR.
- Visit summary and care plan. No patient should leave a call wondering what happened. Each visit ends with a structured summary — impression, medications, referrals, follow-up timing — saved to the patient’s history in plain language.
- A support channel. When something breaks, the provider and patient need to be one tap from a human (or a competent AI agent). As we learned while building AceCancer, a product holding the attention of patients, caregivers, and medical staff at once is a platform with no path to help when any of those three need it.
Note: Sending a standard prescription to a pharmacy is relatively straightforward. The complexity comes when you need to handle controlled substances, which requires EPCS certification and full compliance with DEA regulations. This is an entirely different level of regulatory overhead. If prescribing isn’t essential to your initial care workflow, it’s often reasonable to leave it out of the first version and introduce it in a later release.
The admin control panel
Your users will not be able to see the admin interface. However, this will affect your compliance status and your ability to demonstrate that the platform can operate securely. There are the things you should know:
- User moderation and access control need to be addressed to enable provisioning and deprovisioning of user accounts. Then, you can specify a user and the degree of access to certain features.
- Payout and payment management needs to be addressed to reconcile the various types of statements, including provider payout, billing, and refund statements. Even a basic level of functionality here already signals something important: that payments are actually flowing through the platform.
- Basic analytics with operational signals, such as completed visits, no-show rates, average length of visits, video quality, and time to connect vs. time waiting (all limited to the user role), will assist you in catching the provider who consistently runs behind schedule.
Two items are typically overlooked when preparing the scope of work for an admin-side analysis: the existence of audit trails of all accesses to protected health information and the existence of patients’ consent records. If your agency is located in most states in the United States, the only thing that will validate a telehealth visit is a documented consent form. A checkbox and a date/time stamp without a supporting audit trail would not be acceptable should a challenge arise.
{{banner}}
Breakdown of telemedicine MVP costs
With the scope defined, the numbers get concrete. These ranges reflect full development — design, build, compliance, and architecture for scaling — not a stripped demo.
Average cost ranges by platform (web vs. iOS/Android mobile)
A provider dashboard is almost always web-based — clinicians work at a desk, on a larger screen, often inside a clinic network. Patients tend to use mobile devices, so you’re primarily dealing with iOS and Android.
Creating two different native applications will roughly double the effort required for front-end development. However, you can reduce costs significantly by using a cross-platform framework, such as React Native. This way, you’ll create a common codebase that can be accessed via both applications.
However, creating just a web-based experience for patients would be even less expensive than these options. During the telehealth experience, patients generally expect to be able to download information to their mobile devices. Most version 1 builds use React Native for the patient-facing app and either React or Angular for the provider/admin side.
The hidden costs: healthcare compliance and data security (HIPAA, GDPR)
When you see a telemedicine MVP priced at $15,000 or $30,000, what’s missing is almost always the regulatory layer. And in healthcare, that layer sets the floor for the entire build.
The architecture itself is defined by compliance from inception to conclusion. All message transmissions (including uploaded data, laboratory reports, and clinical notes) are encrypted using:
- AES-256 when data is idle;
- TLS 1.2 when data is transmitted;
- SRTP for audio/video streams.
Multi-factor authentication has been mandatory for all clinician accounts since the 2026 HIPAA Security Rule revisions. All vendors who handle sensitive information (PHI) must also use audit logging and consent-to-treat. The EU’s General Data Protection Regulation establishes additional requirements for healthcare organizations processing data outside the end user’s location, regardless of the end user’s location. Additionally, certain Middle Eastern jurisdictions have regulations that impose data residency requirements.
Teams that treat HIPAA and GDPR as a final checklist routinely discover they need to rebuild core data infrastructure. That rebuild — not the original feature — is where budgets blow up. Costing compliance in from the start is the cheapest version of it you’ll ever buy.
Cost differences among in-house teams, agencies, and offshore development
The same scope costs wildly different amounts depending on who builds it:
- In-house team. Maximum control and continuity, highest fixed cost. Hiring HIPAA-literate engineers, a healthcare-savvy designer, QA, and a compliance consultant before you’ve validated the product is a heavy bet — and slow, given healthcare hiring timelines.
- Dedicated team. Companies with experience bringing regulated healthcare products to market have the expertise and established vendor relationships gained from previous projects in this field. Therefore, although you will pay more than the typical offshore rate, you will avoid the cost of a complete rebuild.
- Offshore / lowest-bid. While the initial bid may seem attractive, it is fraught with risk. Firstly, you will receive an inexpensive project. Then you will incur additional costs to repair any compliance or data architecture deficiencies that arise during your initial audit. In a regulated environment, the contractor with the lowest price often ends up costing the client more than the next lowest-priced contractor.
When speed of validation and compliance accuracy are the primary factors, previous experience of completing the task generally results in better overall pricing and quality. This is precisely why healthtech companies use this methodology to develop their MVPs and telemedicine apps.
Telemedicine MVP timeline overview
Typically, a focused MVP takes about 10–14 weeks to complete. The integration depth and scope clarity are the main factors affecting the overall timeline. Let’s take a closer look at those timelines.
The discovery and UI/UX prototyping phase (weeks 1–4)
This process establishes the foundation for all subsequent phases. Before making any design decisions, you should establish who will be using your product, how it will be used in a clinical setting, and its regulatory scope. Conducting this discovery process before designing your product reduces the likelihood that you will have to rebuild it several months later due to an unexpected design issue.
This discovery-style work will produce three outputs: a defined first care journey, a compliance floor and ceiling, and prototypes tested against accessibility constraints that will affect your target audience. Because the limits of healthcare UX and traditional product design differ, accessibility should not be treated as a final polishing step.
Backend architecture and core development (weeks 5–12)
Three layers come together here: a secure backend for data and APIs, the patient and provider front ends, and third-party integrations for video, messaging, and payments. Compliance controls are built into the architecture from the start rather than bolted on — the encryption, role model, audit logging, and BAA-backed vendor stack described above. This is the longest stretch, and the one most affected by how cleanly the scope was frozen in discovery.
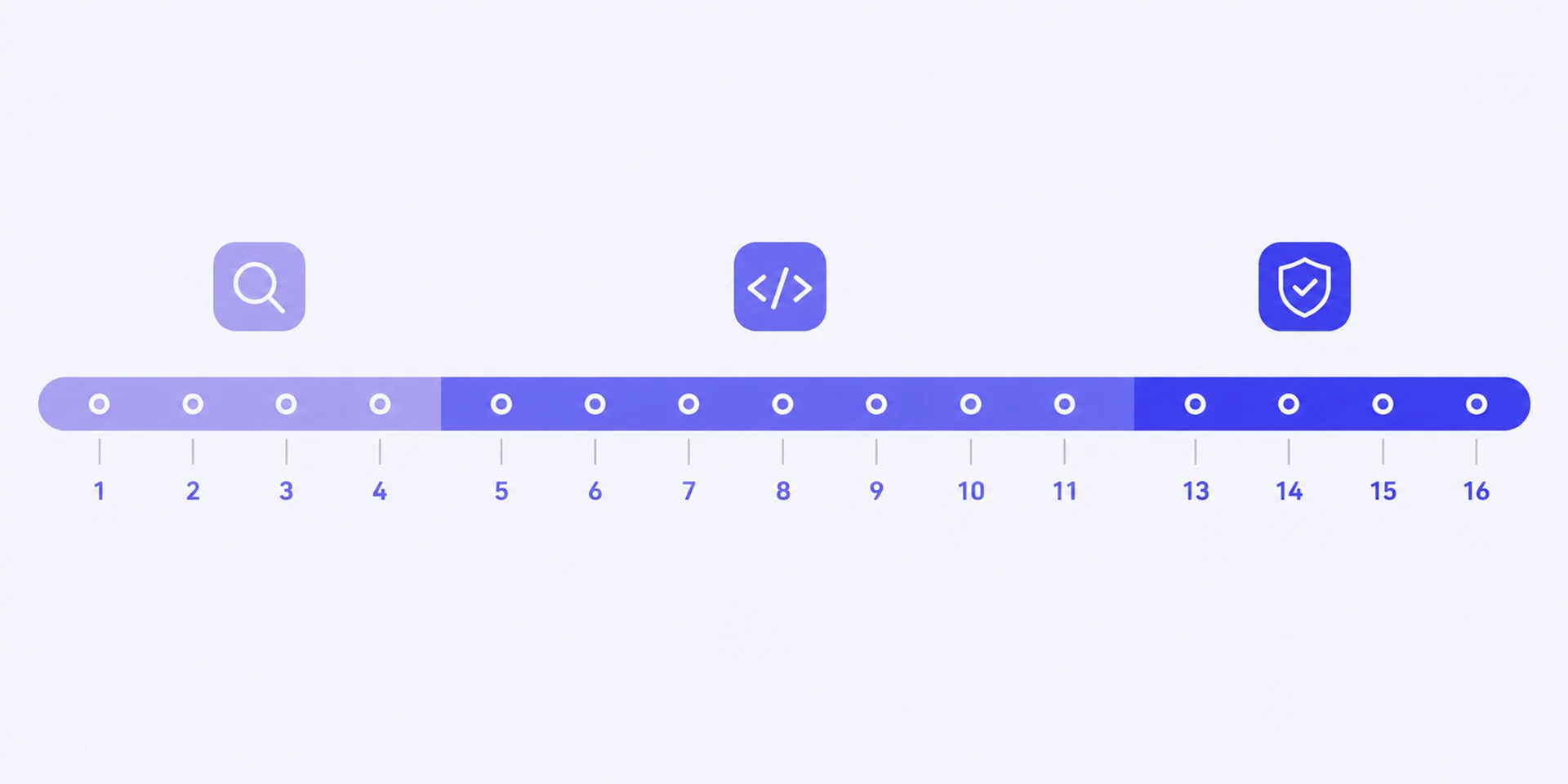
Testing and compliance audits (weeks 13–16)
Functionality testing is the “least complicated” part of a product’s journey. However, when developing a product for the health care industry, the need for security reviews, penetration testing, compliance checks, and additional load testing adds more layers of scrutiny prior to launch. It is critical to test all layers of a product prior to launch so it can withstand the rigors of real, visible patient use. Verifying each layer or component before launch is what differentiates a product that will successfully pass its first significant audit from one that will fail public scrutiny.
What real users tell you after MVP launch
Delivering a narrow product to users allows you to observe exactly how real-world clinicians and patients will use the product (completed appointments, missed appointment rates, where users stop using it, and which features remain unused). By analyzing signals from these real users, you’ll be able to determine exactly which new features to add. The primary function of keeping v1 narrow is to provide the most inexpensive method possible for determining your next expensive feature additions.
Planning your post-launch feature roadmap
When you validate the core set of features, you’ll need to evaluate the delayed feature set according to its validated level of demand:
- Payment and E-Prescription;
- Connected Device Vitals and Remote Monitoring;
- EHR integrations with a partner’s requirement;
- Artificial Intelligence with measurable time saves.
Each phase will be funded with the evidence from the preceding phase. Remote monitoring shows why these steps are important: on the cloud-based RPM platform we designed, we provide care teams with a way to merge device readings into a visual format. This allows care teams to proactively identify deteriorating patients and decrease readmissions — an example of a valuable data layer once the core visit flow has been established.
Consider that the total cost of ownership includes subscriptions to cloud-based providers, hosting services, security updates, and ongoing compliance costs. The budget should account for all of these expenses at launch and continue to allocate funds for them on an ongoing basis. Book a 30-minute call, and we’ll give you a clear breakdown of scope, risks, and cost for your specific care journey.
It’s not the price, it’s the scope
The number on your telemedicine MVP isn’t set by a price list. It’s set by scope — by which of those features you put in version one, how much compliance your jurisdiction demands, and whether you build the integrations now or design for them later. When you get the scope right, the $80K–$120K lean tier is a real, shippable product. Get it wrong, and you pay the rebuild tax no matter what the original quote said.
FAQ
Why invest in branding services services services?
How much does a telemedicine MVP cost?
You can expect to spend between $80,000 and $120,000 for a lean, compliant telemedicine MVP. This price includes secure video conferencing, messaging, scheduling, authentication, and basic profiles on patients in approximately 10-14 weeks. If you add the ability to accept payments, integrate e-prescribe, and build a patient portal, the overall total will be between $120,000 and $180,000. If you also add EHR integration, remote monitoring capabilities, and AI features, the overall total will range between $180,000 and $300,000.
How long does it take to build a telemedicine MVP?
Typically, it takes about 10 to 14 weeks to develop an MVP because it requires approximately 4 weeks for design, 6 to 8 weeks to develop your main functions and features, and another 3 to 4 weeks for testing to ensure compliance. If your platform has a lot of existing EHR integration connections or requires enterprise-level approvals, this will take approximately 6 to 9 months or more.
What affects the telemedicine MVP cost the most?
The two key areas that have the greatest impact on the cost of telemedicine MVPs are the complexity of integrations and the clarity of the defined scope. The biggest variable is connecting with legacy EHRs, followed by how much compliance is required by your state and how disciplined you are about leaving non-essential functionality out of v1. Over-scoping the first release is typically the primary reason for having large changes in budget and timelines.
Can I build a HIPAA-compliant telehealth MVP under $80k?
Yes, it is possible in some cases, but it’s uncommon to build a fully HIPAA-compliant telemedicine MVP for under $80,000 without significant trade-offs. Many low-cost estimates leave out key compliance requirements. Yet, if compliance is not built in from the start, you’ll almost always end up paying more later to redesign the system.
How is a telehealth MVP different from a regular app MVP?
MVP of consumer apps can ship rough and iterate in a public fashion, but a telehealth MVP cannot ship that way and therefore takes longer to ship, due to the handling of protected health information (PHI). The Telehealth MVP must meet compliance and security requirements on day 1 to be legal for launch (the regulatory floor sets a higher bar for a healthcare MVP than for a regular app with similar features).